Blog
Exogenous steroid and adrenal suppression
- 30 March 2021
- Posted by: Aneela Tehseen
- Category: Education

EXOGENOUS STEROID AND ADRENAL SUPPRESSION
REFERENCE TO NATIONAL PATIENT SAFETY ALERT (AUG 2020)
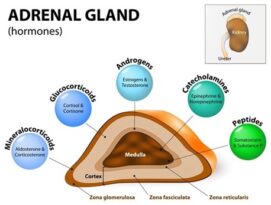
To understand impact of exogenous steroid on hormones excreted by adrenal glands let’s briefly look at adrenal glands:
Adrenal glands are small triangular shaped glands located on top of both kidneys. These glands are a part of endocrine system. Cortex of adrenal glands produces Glucocorticoid (Cortisol), Mineralocorticoid (Aldosterone) and precursors for sex hormones (Androgens and Oestrogens). The Whereas Medulla of adrenal glands produces Catecholamines (Adrenaline, Noradrenaline).
Within human body the Hypothalamus-Pituitary-Adrenal system exhibits a smart negative feedback system that self-regulates; as explained below:

With regards to concerns of lower levels of adrenal hormones and its impact on patients’ life one must appreciate how important adrenal hormones are in daily life and in critical situations such as medical emergencies.
Cortisol has several important roles in body including regulating metabolism of fats, proteins and carbohydrates; regulations of BP; causes a rise in blood sugar levels; reduces bone formation; reduces inflammation; and regulate sleep/awake cycle.
Aldosterone maintains BP via Sodium/potassium and water balance. It promotes more sodium and water absorption alongside potassium excretion.
Normal adrenal gland responds to serious illness by making up to 10 times more cortisol than it usually makes. It automatically makes as much as the body needs. Now let’s consider a patient who lacks this ability to do so. And there are two reasons why an individual might lack the ability:
- Primary adrenal insufficiency. Such as Addison’s disease. This is an autoimmune condition. Less common causes include infiltration like cancer and infections like AIDS, TB etc.
- Secondary renal insufficiency. Most common cause is exogenous steroid administration; Radiotherapy related hypothalamic/ pituitary suppression; Steroid producing tumours; certain medication e.g. Chlorpromazine etc.
Management of patient with primary adrenal insufficiency includes both Glucocorticoid and Mineralocorticoid supplementation. Hydrocortisone is the mainstay of the therapy for Glucocorticoid replacement (adult dose varies from 15-30mg/day in 3 divided doses with the highest dose to be taken in the morning to mimic natural diurnal rhythm). During minor illness like an infection patient is advised to triple the dose and during major illness (such as planned surgery, suspected adrenal crises) dose is increased by 10 times. Fludrocortisone is used for Mineralocorticoid replacement (adult dose varies from 50-200mcg/day based on weight/ activity levels etc.) Dose adjustments are guided by regular monitoring of Sodium/Potassium levels, BP and blood sugar level.
Now let’s explore secondary adrenal insufficiency such as due to exogenous steroid administrations. It is obvious that systemic steroids carry the highest risk to suppress adrenal gland vs other routes of administration. However, it has been found that high dose of inhaled steroids or potent/ very potent steroids applied to rectal/genitals or large body areas are also able to trigger negative feedback and hence suppress adrenal glands.
Symptoms of adrenal suppression:
Adrenal suppression due to glucocorticoid administrations are often vague and can be misunderstood for other illnesses. Below are some symptoms of adrenal suppression, please note these are NOT symptoms of adrenal crisis.
- Weakness/fatigue
- confusion
- Malaise
- Nausea/ Vomiting
- Diarrhoea
- Abdominal pain
- Headache (usually in the morning)
- Fever
- Anorexia
- Weight loss
- Myalgia
- Arthralgia
- Poor linear growth in children
- Delayed puberty in children
- Psychiatric symptoms
Symptoms of adrenal crisis:
Crisis occurs when the physiological demand for these hormones exceeds the ability of adrenal glands to produce them, most often in patients with chronic adrenal insufficiency when subject to an intercurrent illness or stress.
- Hypotension
- Unexplained hypoglycaemia
- Acute abdominal pain
- Hyponatraemia
- Hypovolemic shock
- Decreased consciousness
- Seizure
- Coma
Distinguishing between primary and secondary adrenal insufficiency: We understand from Hypothalamus-Pituitary-Adrenal axis that adrenal insufficiency must be primary if there is plenty ACTH and adrenal glands are still unable to respond by generating Cortisol, and Aldosterone. On the other hand if ACTH is low/ very low then we know that the system is operating under negative feedback and adrenal glands are just not getting the message to generate endogenous hormones (cortisol and Aldosterone etc.)
If adrenal suppression is suspected morning Cortisol (highest levels are around 8:00-9:00 am, although specialist interpretation needed for shift workers/ pregnant ladies/ those taking COC pill or HRT pills). Each lab may use different measuring unit, however, if you get results in nmol/L and the results are ≤ 100nmol/L, it calls for urgent investigation and/or admission. And if the results are between 100-500nmol/L, patient should be referred to endocrinology.
ACTH levels are ↑ in primary adrenal insufficiency and normal or ↓ in secondary adrenal insufficiency. If it’s still unclear a short ACTH stimulation test (Synacthen) can be used. For the test patient needs to have an early morning pre-test blood sample taken, and then a dose of Synacthen (Tetracosactide, a chemical copy of ACTH) is administered. 30 minutes later another blood sample is taken to check cortisol levels. A cortisol level ≥420nmol/L indicates adequate adrenal response. Levels lower than this would either suggest Addison’s disease or marked adrenal atrophy secondary to prolonged absence of ACTH.
Do other drugs affect Glucocorticoids exposure?
Yes, other drugs when co-administered may increase or decrease the exposure to glucocorticoids. Some examples are explained below:
|
Name of the Drug |
Effect on exposure of Glucocorticoid |
Mechanism |
|
Anticonvulsants (Carbamazepine, Phenytoin, Phenobarbital |
↓ |
Via inducing metabolic liver enzymes hence metabolising glucocorticoid at faster rate |
|
Antifungals (Itraconazole, Ketoconazole) |
↑ |
Inhibition of CYP3A4. Prednisolone is not affected |
|
Antibacterial (Macrolides) |
↑ |
Inhibition of CYP3A4 |
|
Antiviral (Ritonavir, Indinavir, Saquinavir etc.) |
↑ |
Extreme inhibition of CYP3A4 |
|
Opiates |
↑ |
Possible direct HPA suppression |
NPSA released in Aug 2020 explains that all patients with primary adrenal insufficiency are steroid dependent. The alert also states that patients receiving steroids for other medical conditions may also develop adrenal suppression. Both of these groups are at risk of developing adrenal crisis in situations of major stressors like medical emergency. It is recommended to identify all adult patients who are at risk of adrenal suppression and be issued with a RED steroid emergency card by their prescribers. An image of the card is shown below:

All prescribers are urged to regularly review prescribing of steroids either as scheduled reviews or at the point of authorising a repeat prescription. Community and hospital pharmacies are not currently required to supply the RED steroid Emergency alert cards, but have been advised to source the supplies in order to enable them to replace patients’ lost/damaged Steroid alert cards.
Who should receive a Steroid Emergency Card?
- Patients who received systemic glucocorticoid course for long-term (longer than 4 weeks) at dose ≥5mg Prednisolone/day. The dose equivalence is explained below:
|
Name of Glucocorticoid |
Equivalent dose/day if received daily for more than 4 weeks requires issue of Steroid Emergency Alert Card |
|
Prednisolone |
≥5mg and for 12 months after stopping the treatment |
|
Methylprednisolone |
≥4mg and for 12 months after stopping the treatment |
|
Hydrocortisone |
≥15mg and for 12 months after stopping the treatment |
|
Dexamethasone |
≥500mcg and for 12 months after stopping the treatment |
|
Betamethasone |
≥750mcg and for 12 months after stopping the treatment |
- Patients who received short courses of systemic glucocorticoids. This group includes those who received repeated short courses (≥ 3) of oral steroids or patients who received 1 week or longer course and has also been on long course of oral steroids within past 12 months.
|
Name of Glucocorticoid |
Equivalent dose/day if received for 1 Week +use of long-term steroid in past 12 months OR ≥3 short courses/6 months requires issue of Steroid Emergency Alert Card |
|
Prednisolone |
≥40mg and for 12 months after stopping the treatment |
|
Methylprednisolone |
≥32mg and for 12 months after stopping the treatment |
|
Hydrocortisone |
≥120mg and for 12 months after stopping the treatment |
|
Dexamethasone |
≥4mg and for 12 months after stopping the treatment |
|
Betamethasone |
≥6mg and for 12 months after stopping the treatment |
- Patients receiving regular inhaled corticosteroids. A dose at which a steroid alert card is needed may be guided by the table below:
|
Name of Glucocorticoid |
Equivalent inhaled dose/day |
|
Beclomethasone |
≥1000mcg and for 12 months after stopping the treatment |
|
Beclomethasone (Extra-fine particles) QVAR, Fostair, Kelhale |
≥500mcg (Also take into account if patient is on MART/ SMART regime) and for 12 months after stopping the treatment |
|
Budesonide |
≥1000mcg (Also take into account if patient is using MART regime for combination inhalers) and for 12 months after stopping the treatment |
|
Ciclesonide |
≥480mcg and for 12 months after stopping the treatment |
|
Fluticasone |
≥500mcg and for 12 months after stopping the treatment |
|
Mometasone |
≥800mcg and for 12 months after stopping the treatment |
Miscellaneous routes of Glucocorticoid administration and need of Steroid Emergency Alert Card:
|
Route of administration |
Frequency of administration |
|
Intra-articular or IM |
≥3 in past 12 months and for 12 months after stopping the treatment |
|
Oral Dexamethasone as antiemetic during chemotherapy |
Repeated courses (Steroid card should be issued at the first cycle of Dexamethasone, when future cycles are anticipated) and for 12 months after stopping the treatment |
|
Use for severe COVID-19 |
Prolonged use (more than 10 days’ use) |
|
Topical potent/ very potent glucocorticoids over large surface area (usage ≥200g/week) |
≥4 weeks and for 12 months after stopping the treatment |
|
Topical potent/ very potent glucocorticoids on rectal/genital area (usage ≥30g/week) |
≥4 weeks and for 12 months after stopping the treatment |
- Other groups of patients who also require issue of Steroid Emergency Alert card: These include any patients who are in receipt of glucocorticoid therapy and are being prescribed long-term courses of Clarithromycin, oral antifungals (Itraconazole, Ketoconazole, Variconazole) and those receiving potent protease inhibitors (Astazanavir, Duranavir, Ritonavir, Saquinavir etc.)
- Where patient is using a dose of glucocorticoid that is less than the thresholds described above but is using multiple routes e.g. inhaled + intranasal + topical, an individual case assessment is required and a Steroid Emergency Alert Card may still be indicated.
References:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3765115/
https://patient.info/doctor/adrenal-insufficiency-and-addisons-disease#nav-6
https://patient.info/doctor/adrenal-crisis
University College of London Hospital: Adrenal insufficiency; Patient safety First; by Dr H.Simpson (Consultant Endocrinologist)