Blog
A Life Interrupted by Progressive MS – What Primary Care Needs to Know

By Jeshni Amblum Almér and Fredrik Lindqvist .
A Brother’s Story: Richard Lindqvist (1967–2020) “Sometimes, life throws you a curveball… one you never saw coming. And in an instant, everything changes.”
This is the story about Richard Lindqvist through the eyes of his brother Fredrik, Richard grew up in the countryside and spent his days working r, working side by side with your brother on the family farm, fixing engines, tinkering with machines, hauling tools, and happiest when his hands were covered in oil and his boots in mud. Richard Lindqvist lived in the Swedish countryside and worked as a car mechanic and part-time firefighter. He was a man who thrived on practical work and was known for his inventiveness and humour. But in 2009, at the age of 41, something began to change. It started with a change in vision, images appeared upside down, colours faded and then there was the extreme fatigue.
“I just felt off,” he reportedly told his family. He developed a persistent throat and sinus infection, a bout of chronic illness that lingered for weeks. His energy waned. He became unusually tired after routine tasks. Subtle changes in gait, clumsiness, and tightness in his legs crept in. It didn’t seem serious at first, perhaps post-viral fatigue, maybe stress. But the symptoms worsened, gradually and relentlessly. That was the beginning of the interruption. The curveball. And what followed was a diagnosis no one saw coming: Primary Progressive Multiple Sclerosis. In 2010, Richard was diagnosed with Primary Progressive Multiple Sclerosis (PPMS). It took at least 2-3years, after repeated visits to his doctor and various specialists. How often have our patients told us a similar story. His condition deteriorated steadily. Over the next ten years, Richard would lose the ability to walk, then to move, and ultimately to care for himself. He died in 2020 at just 53 years old. His brother Fredrik, devastated by the lack of treatment options, started MS-fonden RICHARD: mot MS, för livet, a foundation dedicated to funding research into progressive MS. Through this, Richard’s legacy lives on. This is Richard’s story, and through it, a reminder of the importance of early recognition, primary care vigilance, and the humanity behind every diagnosis
The Bigger Picture: MS and the Expanding Role of Primary Care
Multiple sclerosis (MS) is the most common non-traumatic neurological cause of disability in young adults, affecting over 130,000 people in the UK. While typically considered a disease of women in their 20s and 30s, cases like Richard’s are a crucial reminder: MS does not discriminate by age or gender, and progressive forms often appear later, especially in men.
Epidemiology and Risk Factors: Where Medicine Meets Environment
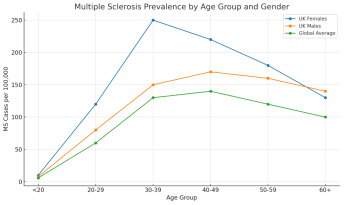 The graph illustrates the estimated prevalence of multiple sclerosis (MS) across different age groups and genders, drawing comparisons between UK-specific and global data. As expected, the highest rates of MS diagnosis in the UK occur among women aged 30–39, aligning with established trends. In contrast, the prevalence in men rises more gradually but remains significant, particularly after the age of 40. This pattern is especially notable in cases of primary progressive MS (PPMS), the very form Richard Lindqvist was diagnosed with at age 41. Globally, the prevalence mirrors this trend, albeit at slightly lower levels across all age bands. Richard’s case highlights a critical and often overlooked demographic: middle-aged men, who are frequently diagnosed later and whose symptoms may missed entirely in primary care. This reinforces the urgent need for early recognition and proactive referral across all age groups, not just in young women, so that individuals like Richard have the best possible chance of timely intervention and support.
The graph illustrates the estimated prevalence of multiple sclerosis (MS) across different age groups and genders, drawing comparisons between UK-specific and global data. As expected, the highest rates of MS diagnosis in the UK occur among women aged 30–39, aligning with established trends. In contrast, the prevalence in men rises more gradually but remains significant, particularly after the age of 40. This pattern is especially notable in cases of primary progressive MS (PPMS), the very form Richard Lindqvist was diagnosed with at age 41. Globally, the prevalence mirrors this trend, albeit at slightly lower levels across all age bands. Richard’s case highlights a critical and often overlooked demographic: middle-aged men, who are frequently diagnosed later and whose symptoms may missed entirely in primary care. This reinforces the urgent need for early recognition and proactive referral across all age groups, not just in young women, so that individuals like Richard have the best possible chance of timely intervention and support.
What is MS
Multiple sclerosis (MS) is a chronic, immune-mediated neurological disorder influenced by a combination of genetic predispositions and environmental factors. Among the most well-established risk factors are infection with the Epstein–Barr virus (particularly in the form of infectious mononucleosis, which can double the risk of developing MS), low serum vitamin D, reduced ultraviolet B exposure, and smoking,which increases MS risk by approximately 50%, potentially explaining its rising incidence among women. Additional contributors include childhood obesity and carriage of the HLA-DRB1*15:01 allele. Clinically, MS presents in several forms. The most common is relapsing-remitting MS (RRMS), marked by episodes of neurological symptoms followed by periods of partial or complete recovery. Over time, RRMS can transition into secondary progressive MS (SPMS), characterised by gradual neurological decline. Alternatively, some patients, like Richard Lindqvist, are diagnosed with primary progressive MS (PPMS), which involves a steady worsening of symptoms from the outset, often with signs such as spastic paraparesis.
In primary care, early recognition of MS is vital but often challenging, as symptoms can be vague or intermittent. Warning signs include unilateral optic neuritis – this was something Richard first encountered. Living in a country with long, dark winters possibly did not help and here again highlights the importance of vitamin D.This follows with steadily increased numbness and tingling, unexplained weakness or ataxia, and cognitive difficulties or fatigue. Red flags for alternative diagnoses include systemic symptoms like fever or rash, onset over the age of 50, and progressive symptoms without prior relapses. If MS is suspected, urgent referral to neurology is essential. Diagnostic investigations include MRI of the brain and spinal cord (to identify dissemination in space and time), lumbar puncture to detect CSF-specific oligoclonal bands, and evoked potentials to assess neural pathway function. The 2017 McDonald criteria allow for earlier diagnosis through imaging and cerebrospinal fluid analysis, enabling earlier therapeutic intervention.
McDonald Criteria
The McDonald Criteria, most recently revised in 2017, provide a structured framework for diagnosing multiple sclerosis (MS) by integrating clinical presentation with MRI and cerebrospinal fluid (CSF) findings. The criteria support diagnosis in patients with typical relapsing-remitting presentations as well as those with progressive symptoms from onset, provided there is sufficient radiological or CSF evidence. This allows for timely intervention, improving long-term outcomes through earlier access to disease-modifying therapies
Key risk factors include:
| Risk Factor | Key Details |
| EBV Infection | Nearly all people with MS are EBV-seropositive. Those who had infectious mononucleosis have double the risk. (Bjornevik et al., Science, 2022) |
| Vitamin D Deficiency | Low UVB exposure is a major risk factor. Richard lived in Sweden, where winters are long and sunlight is scarce—compounding his risk. |
| Smoking | Increases MS risk by ~50%. May explain rising rates among women. |
| Obesity in Adolescence | Particularly relevant to girls. Raises inflammatory cytokines. |
| Genetics | HLA-DRB1*15:01 allele increases risk over 6-fold in homozygotes. |
| Microbiome | Recent research links gut bacteria (Clostridium perfringens, Lachnoclostridium) to neuroinflammation in MS. (PNAS, 2024; JCI, 2023) |
Clinical Course and Subtypes
Multiple sclerosis (MS) is now widely recognised as a spectrum disorder, rather than a condition with rigid subtypes. It ranges from relapsing-remitting MS (RRMS), characterised by periods of attacks and recovery, to secondary progressive MS (SPMS), which develops from RRMS and involves a steady functional decline. A less common but often more debilitating form is primary progressive MS (PPMS), which is marked by a gradual worsening from onset without remission. This was the type diagnosed in Richard Lindqvist, whose subtle early symptoms—chronic sinus and throat infections, fatigue, and limb stiffness, were typical of what may initially present in general practice, yet they were not immediately recognised as neurological in nature. Richard’s late diagnosis at age 41 highlights the urgent need for early suspicion and referral, especially in patients who fall outside the typical MS demographic of younger women.
Like many people with MS, Richard’s condition likely arose from a complex interplay of genetic and environmental factors. One significant risk factor is Epstein–Barr virus (EBV); virtually all MS patients have been infected, and a study by Bjornevik et al. (Science, 2022) found a 32-fold increased risk following symptomatic EBV infection such as glandular fever. Vitamin D deficiency, particularly in northern latitudes like Sweden where Richard lived, may have further increased his susceptibility. Sweden has long, dark winters and there is an opportunity in primary care to highlight the importance of vitamin D. Smoking, if present, could have contributed to both the disease onset and its rapid progression, risk increases by up to 70%. Additionally, genetic predispositions such as carrying the HLA-DRB1*15:01allele or having a family history may have played a role. Other contributing factors could include mid-life obesity, exposure to organic solvents in occupational settings like mechanics or firefighting (Richard’s professions), and the fact that men with MS are more likely to experience a progressive and rapidly deteriorating course.
Richard’s story serves as a powerful case study underscoring the importance of vigilance in primary care, not just for classical MS presentations, but also for atypical or insidious symptoms in older adults and men, who are often diagnosed later and have more aggressive disease trajectories.
Possible Early Symptoms He May Have Experienced
In late-onset MS, the disease more commonly presents with motor or sensory symptoms, often mistaken for musculoskeletal or age-related conditions. Some early signs may have included:
| Symptom | Explanation |
|
Tingling or numbness |
Usually in limbs; often asymmetric |
|
Muscle weakness |
Especially in the legs; may be progressive rather than relapsing |
|
Gait problems / unsteadiness |
Balance issues or foot drop due to spinal cord involvement |
|
Bladder issues |
Urinary urgency, frequency, or retention may appear early |
|
Visual disturbance |
Optic neuritis is less common in late-onset MS but still possible |
|
Fatigue |
A hallmark symptom, sometimes the only one initially |
|
Spasticity |
Muscle stiffness or spasms, particularly in the legs |
Symptoms are also more likely to be attributed to other causes (e.g., stroke, arthritis, neuropathy), which can delay diagnosis and treatment. If diagnosis was delayed, inflammation and neurodegeneration may have progressed unchecked.
Common Early Symptoms:
-
- Unilateral optic neuritis
-
- Tingling or numbness in dermatomal distribution
-
- Fatigue, ataxia, muscle stiffness
-
- Subtle cognitive issues
Red Flags That Suggest Alternatives:
-
- Systemic illness (fever, rash)
-
- Age >50 at onset (consider other causes, but don’t exclude MS)
-
- No previous relapses or MRI findings
Referral and Workup
Recent advances in microbiome research have introduced compelling evidence that certain gut bacteria and their toxins may play a contributory role in the development and progression of multiple sclerosis (MS). A landmark study published in The Journal of Clinical Investigation identified Clostridium perfringens strains producing epsilon toxin,found in higher abundance in patients with MS. In preclinical models, this toxin disrupted the blood, brain barrier, facilitating immune cell infiltration and subsequent demyelination, mimicking MS pathology. This represents the first time a specific bacterial toxin has been proposed as a plausible environmental trigger of MS, though not a direct cause. This was highlighted in another 2024 study. When these gut microbes were transferred to genetically susceptible mice, the animals developed MS-like disease, with a stronger response observed in females, mirroring the gender disparity seen in human MS prevalence. Additional findings show that a reduced Bifidobacterium-to-Akkermansiaratio may be linked with more severe disease outcomes. These findings support the gut–brain axis hypothesis and open new avenues for microbiome-based therapies. While causality remains unproven, this evolving research landscape offers a potential explanation for atypical cases like that of Richard Lindqvist, who developed primary progressive MS in his early forties, following recurrent sinus and throat infections. Richard’s experience, highlights the need for heightened clinical awareness of environmental and microbial risk factors in adult-onset MS, especially among males presenting outside the typical diagnostic window.
Management and Monitoring in General Practice
While neurologists typically manage disease-modifying therapies (DMTs), general practitioners play a crucial role in ongoing care. This includes monitoring for comorbidities such as cardiovascular disease, osteoporosis, and mental health disorders; supporting adherence to treatments; and managing symptoms like fatigue (with lifestyle changes or off-label use of modafinil), spasticity (baclofen and physiotherapy), neuropathic pain (gabapentin, amitriptyline), and bladder or bowel dysfunction. Depression and anxiety are also common and should be proactively addressed. According to NICE guideline CG186, care for people with MS should be holistic and person-centred, incorporating early rehabilitation, access to psychological support, and self-management education. While neurologists initiate DMTs, primary care teams are key to:
Disease-Modifying Therapies (DMTs)
Disease-modifying therapies (DMTs) have significantly reshaped the landscape of multiple sclerosis management, with over a dozen licensed options now available in the UK. These include injectable treatments such as interferons and glatiramer acetate, oral agents like fingolimod, teriflunomide, and dimethyl fumarate, and monoclonal antibodies including ocrelizumab, natalizumab, and alemtuzumab. The therapeutic goal is to achieve No Evidence of Disease Activity (NEDA)—a composite measure based on clinical symptoms, MRI activity, and biomarkers like neurofilament light chain (NFL). Importantly, newer therapies such as ocrelizumab have been approved for primary progressive MS (PPMS), the form that affected Richard Lindqvist. While these treatments may have come too late to alter the course of Richard’s illness, they offer renewed hope for future patients diagnosed with progressive MS. These advancements underscore the value of early detection and timely intervention, particularly as treatment strategies continue to evolve for forms of MS once considered untreatable.
Psychosocial Impact
The impact of multiple sclerosis (MS) extends far beyond the central nervous system, deeply affecting patients’ emotional wellbeing, relationships, employment, and sense of autonomy. Individuals like Richard Lindqvist, who developed primary progressive MS (PPMS) in his early forties, often face a rapid decline in physical abilities, leading to profound psychological and social consequences. Depression and anxiety are common, with estimates suggesting up to 50% of people with MS experience significant mood disturbances during their illness. Many also face social isolation, especially when mobility is reduced or speech and cognitive difficulties emerge. Loss of employment and role identity, as in Richard’s case, where he could no longer continue his work as a mechanic and part-time firefighter, further compounds the emotional burden. In progressive cases, patients may also require early support with care needs, mobility aids, and even safeguarding measures if they become vulnerable. Richard tells his own experience of navigating the health and care system, his relationship with his own family and spouse and the impact his illness had on them. Here, the role of primary care is pivotal. General practitioners and practice nurses are well positioned to provide routine mental health screening, offer or coordinate psychological support, and facilitate access to local services such as MS nurses, occupational therapy, physiotherapy, and counselling. In advanced disease stages, they also support palliative care discussions, advanced care planning, and can act as a consistent point of contact in a fragmented care system. Delivering compassionate, person-centred care is not just clinical best practice, it is a vital act of humanity for people whose lives have been interrupted and reshaped by MS. The disease reaches beyond the individual, to the very community from which he is a part.
Research and Future Frontiers in MS Management
Ongoing research in multiple sclerosis (MS) is uncovering promising strategies that could redefine both prevention and treatment, especially for progressive forms like the one experienced by Richard. While current disease-modifying therapies (DMTs) focus on slowing progression and reducing disease activity, future research aim to identify and interrupt the underlying disease process, or even prevent MS onset altogether. One of the most exciting areas is stem cell therapy, particularly autologous haematopoietic stem cell transplantation (AHSCT). Clinical trials and observational studies, such as the MIST trial, have demonstrated sustained remission in patients with aggressive forms of relapsing MS, and emerging data suggest potential benefit for primary progressive MS (PPMS) as well. However, its use remains limited to highly selected patients due to risks and cost. Another major research avenue involves Epstein–Barr virus (EBV), now strongly implicated as a trigger in MS pathogenesis. Based on findings from Science (2022), where a 32-fold increased MS risk was observed following EBV infection, EBV vaccines are now in early-phase trials. These could one day offer primary prevention, especially in high-risk individuals such as those with family history or specific genetic markers like HLA-DRB1*15:01.
The role of the gut microbiome is also gaining attention. Studies, including twin research and microbiota transplantation in animal models, suggest that certain bacterial strains may influence immune regulation and MS onset. Interventions such as probiotics or faecal microbiota transplantation (FMT) are now under investigation to explore whether modulating the gut flora can reduce inflammation or delay disease progression. Lastly, high-dose vitamin D supplementation is being studied in both high-risk individuals (e.g., first-degree relatives of MS patients) and those with early MS. Given its immunomodulatory role and strong epidemiological link to MS incidence,especially in northern latitudes like Sweden, where Richard lived, this simple intervention may become a low-cost, widely accessible tool in future MS prevention strategies. These advances may have come too late to benefit Richard, but they offer some hope for future patients, particularly those at risk of, or newly diagnosed with, progressive MS. As research continues, the integration of immunology, virology, microbiology, and genetics will be essential in moving MS care from symptom management to true disease prevention.
Conclusion: Honouring Richard, Informing Practice
Richard Lindqvist’s story is a sobering reminder that MS can affect anyone, and that primary progressive MS, though less common, often carries the greatest burden. Primary care professionals are not just gatekeepers, they are partners in the lifelong journey of those with MS. From spotting that first subtle symptom to coordinating complex care plans, the role of GPs, nurses, and allied professionals is pivotal. Richard’s voice, though silenced by disease, continues to inspire change. Through education, vigilance, and compassion, we can ensure that others like him are diagnosed earlier, managed better, and supported with dignity.