Blog
Testosterone Beyond Libido: A Guide to Metabolic, Cardiovascular and Cognitive Health
Testosterone is an important hormone in both men and women, although it is present in much higher levels in men. In men, it is produced mainly by the testes and is essential for the development of male reproductive organs, maintenance of libido, sperm production, muscle mass, bone density, and overall energy and wellbeing. In women, smaller amounts are produced by the ovaries and adrenal glands, where testosterone contributes to sexual desire, bone strength, muscle maintenance, mood regulation, and cognitive function. Rather than being solely a “male hormone,” testosterone plays a role in metabolic health, body composition, and psychological wellbeing in both sexes. Imbalances—either too low or too high—can lead to symptoms such as fatigue, reduced libido, mood changes, loss of muscle mass, or, in women with excess levels, features such as acne or hirsutism. Understanding testosterone as a hormone relevant to both men and women helps clinicians take a more holistic approach when assessing symptoms related to hormonal health.
Testosterone Across the Life Course
Before Birth (Foetal Development): Testosterone is essential for forming male reproductive organs such as the penis, scrotum, and prostate. If levels are insufficient at this stage, normal sexual development may be affected.
During Puberty: A natural rise in testosterone drives the changes seen in adolescence:
-
- Deepening of the voice
-
- Growth of facial and body hair
-
- Increase in muscle mass and strength
-
- Development of sexual function and libido
Key Roles of Testosterone in Adult Health
- Testosterone supports multiple body systems
-
- Regulates libido, erectile function, and sperm production (via action on Sertoli cells), making it essential for fertility.
-
- Promotes protein synthesis in muscle. Low levels can contribute to sarcopenia (loss of muscle mass and strength).
-
- Stimulates bone-building cells (osteoblasts), helping maintain bone density and reduce the risk of osteoporosis.
-
- Plays a role in motivation, vitality, and overall quality of life.
Why Recognition Matters
- If untreated, testosterone deficiency can contribute to:
-
- Reduced libido and sexual dysfunction
-
- Infertility
-
- Fatigue and low mood
-
- Anaemia
-
- Loss of bone density (osteoporosis)
-
- Reduced muscle mass and strength
- Testosterone is not just a reproductive hormone, it is a key regulator of physical, metabolic, and psychological health. Understanding levels, symptoms, and appropriate investigation is essential for identifying men or women who may benefit from further assessment.
How Testosterone Deficiency Affects Lipid Profiles and Contributes to Atherosclerosis
- Low testosterone is associated with an unfavourable lipid profile and increased cardiometabolic risk. Men with testosterone deficiency often show higher levels of LDL (‘bad’) cholesterol and triglycerides, alongside reduced or less effective HDL(‘good’) cholesterol. These changes promote a pro-atherogenic state, meaning cholesterol is more likely to accumulate within blood vessel walls and contribute to plaque formation. In addition, low testosterone is linked to increased visceral (abdominal) fat, which releases inflammatory mediators that further disrupt normal lipid metabolism and increase cardiovascular risk.
How does Testosterone Supports Normal Lipid Regulation
- Testosterone plays an important role in maintaining healthy lipid balance through several metabolic mechanisms. It helps regulate fat distribution by limiting visceral fat accumulation, which reduces inflammatory signalling and improves how the body processes lipids. Testosterone also influences liver function, supporting the regulation of cholesterol production, transport, and clearance. Furthermore, it enhances insulin sensitivity, allowing better utilisation of glucose and reducing the release of excess fatty acids that can raise triglyceride levels. Its anti-inflammatory effects also help stabilise metabolic pathways involved in lipid handling.
Clinical Significance
- Testosterone should be viewed as a metabolic as well as a reproductive hormone. Adequate levels contribute to healthier cholesterol regulation, body composition, and cardiovascular protection.
- When levels are low, these regulatory mechanisms weaken, increasing the likelihood of dyslipidaemia, metabolic syndrome, and long-term cardiovascular disease.
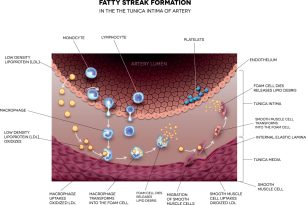
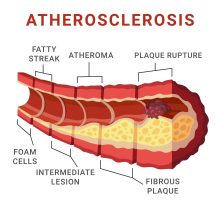
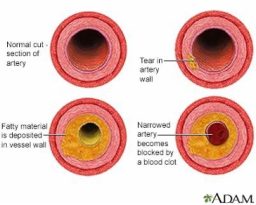
LDL Oxidation and Plaque Formation (Atherosclerosis)
-
Key points shown in this diagram:
- LDL (“bad cholesterol”) enters the artery wall and becomes damaged (oxidised).
- The body treats this as injury and sends immune cells to the area.
- These cells absorb the cholesterol and form fatty build-up called plaque.
- The plaque narrows the artery, reducing blood flow.
- Narrowed arteries increase the risk of heart attack and stroke.
Depression and Low Testosterone
- There is a strong association between low testosterone levels and depression. Men with hypogonadism often report symptoms such as low mood, lack of motivation, fatigue, and anhedonia (loss of interest or pleasure). Testosterone influences neurotransmitters such as dopamine, serotonin and GBA which regulates mood and motivation. Low levels or a deficiency can results in low mood, lack of motivation and anhedonia. Our bodies response to stress is regulated by the hypothalamic-pituitary-adrenal (HPA) axis. Low testosterone can lead to an increase in activity of the HPA axis causing elevated levels of cortisol (sometimes known as the stress hormone) and chronically high levels of cortisol can contribute to depression and anxiety. Testosterone also increases the proteins needed for growth and survival of neurons and low levels of this protein is linked with depression and cognitive decline.
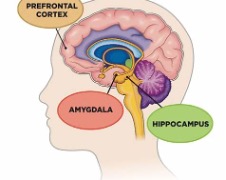
- The amygdala is the brains ‘threat detector”. It rapidly scans for danger and activates emotional and physiological responses to stress. When it becomes overactive (hyperactive):
- The brain perceives threat more easily, even when none exists.
- This is linked to anxiety, low mood, irritability, and heightened stress sensitivity.
- Testosterone helps keep that alarm from becoming too sensitive. Hence, when testosterone is low, the alarm fires more easily, the stress system releases more cortisol, and over time this can contribute to low mood, fatigue, and reduced resilience.
Hippocampus, Memory & Cognitive Decline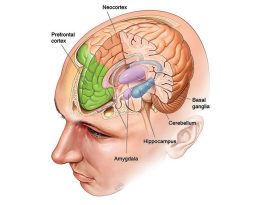
- The hippocampus is the part of the brain that helps us:
-
- Form new memories
-
- Learn new information
-
- Stay mentally sharp
It is one of the first areas affected in Alzheimer’s disease, where it gradually shrinks.
How Testosterone Supports your memory
Testosterone supports the growth and repair of neural connections, helping the brain adapt and maintain memory pathways. It acts as a brain maintenance hormone, supporting metabolic activity, vascular health, and neuronal repair in regions essential for cognition. Chronic deficiency, especially alongside vascular risk factors, metabolic syndrome, or inflammation, may contribute to an environment where cognitive decline progresses more readily. Low testosterone in men has been linked to a higher risk of cognitive decline and conditions such as dementia and Alzheimer’s disease. In men who are truly testosterone-deficient, treatment can lead to some improvement in memory and thinking skills, although benefits in areas like attention or spatial ability are less consistent. However, the benefits seen in studies are usually modest, and results vary depending on factors such as age, starting testosterone levels, and length of treatment.
Testosterone and Energy: Why It Matters for Motivation and Wellbeing
Testosterone plays an important role in motivation and energy by influencing dopamine, a brain chemical responsible for drive, reward, and focus. When testosterone levels are adequate, dopamine signalling works more effectively, helping individuals feel motivated, engaged, and mentally energised. Low testosterone can reduce this activity, leading to symptoms such as lack of motivation, reduced enjoyment, and persistent fatigue. In addition, lower levels may contribute to reduced muscle strength, poorer stress regulation, and decreased physical endurance, all of which can add to feelings of tiredness. As a result, testosterone acts as a regulator of both mental and physical energy, and deficiency can present as low drive and ongoing fatigue rather than just sexual symptoms.
Early Morning Testing: Understanding Diurnal Variation
Testosterone is not constant throughout the day — it follows a natural daily pattern. In healthy men, levels are highest in the early morning, usually between 7:00 AM and 11:00 AM, and then gradually fall as the day goes on. This rise and fall are more noticeable in younger men and becomes less marked with age as the body’s internal clock changes. This daily rhythm is important in clinical practice. Because testosterone peaks in the morning, this is the best time to measure it to get an accurate picture of hormone levels. Testing later in the day, when levels have naturally dropped, can make testosterone appear falsely low. Research has shown that many men who test low initially may have normal levels when the test is repeated in the morning, highlighting the importance of correct timing when assessing testosterone.
Levels (LH and FSH): Differentiating Between Primary and Secondary Hypogonadism
There are two hormones called Luteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH) that released by the pituitary gland and they regulate the function of the testes. Measuring these hormones helps to differentiate between primary hypogonadism (a problem with the testes) and secondary hypogonadism (a problem with the hypothalamus or pituitary gland). In primary hypogonadism, the problem lies in the testes themselves. Blood tests show low testosterone but high LH and FSH levels because the pituitary gland is trying to stimulate the testes to produce testosterone, but the testes are not responding properly. Common causes include genetic conditions such as Klinefelter syndrome, inflammation of the testes (orchitis), and damage from radiation or chemotherapy. In secondary hypogonadism, the testes are capable of working, but the signals from the brain are inadequate. Blood tests show low testosterone with low or normal LH and FSH levels, indicating a problem in the hypothalamus or pituitary gland, which control hormone production. Common causes include pituitary tumours, obesity, certain medications (such as opioids or long-term steroids), and chronic illness.
Primary hypogonadism is a testicular problem, whereas secondary hypogonadism is a signalling problem from the brain.
Understanding SHBG and Why It Matters
Sex Hormone-Binding Globulin (SHBG) is a protein in the blood that binds to testosterone. When testosterone is attached to SHBG, it cannot be used by the body. Only the free (unbound) testosterone is biologically active and able to affect tissues such as muscle, bone, and the brain.
SHBG levels can change in certain conditions:
-
- Obesity tends to lower SHBG
-
- Thyroid disorders affect SHBG (high in hyperthyroidism, low in hypothyroidism)
-
- Liver disease can alter SHBG production
-
- Ageing usually increases SHBG levels
Why Testing SHBG is Important
Measuring total testosterone alone does not always show how much usable testosterone is available. By checking SHBG, clinicians can calculate free testosterone, which gives a more accurate picture of hormonal status. For example, in older men SHBG may be high, so total testosterone can appear normal while free testosterone is low, leading to symptoms of deficiency. Therefore, SHBG testing is particularly helpful when blood results do not match the patient’s clinical symptoms.
Summary of Key Blood Tests in Assessing Testosterone Deficiency
| Test | Clinical Purpose | Why It Matters in Practice |
| Early Morning Total Testosterone | Measures testosterone at its natural peak (diurnal rhythm) | Provides the most accurate reflection of true hormonal status and avoids falsely low readings later in the day |
| Repeat Testosterone Measurement | Confirms persistently low levels | Reduces the risk of misdiagnosis caused by normal biological variation or temporary suppression |
| LH and FSH (Gonadotropins) | Distinguish between primary (testicular) and secondary (pituitary/hypothalamic) hypogonadism | Helps identify the underlying cause and directs further investigation and management |
| Sex Hormone-Binding Globulin (SHBG) | Evaluates how much testosterone is bound vs. available | Allows calculation of free testosterone and can uncover deficiency when total testosterone appears normal |
Clinical Note:
These tests should always be interpreted alongside symptoms, as biochemical results alone do not define hypogonadism.
The Role of GPs in Testosterone Management in Primary Care
General practice (GP) plays a central role in the diagnosis, management, and monitoring of testosterone deficiency in men, particularly in distinguishing between primary hypogonadism (PH) and secondary hypogonadism (SH). They are often the first point of contact for patients presenting with symptoms such as fatigue, low libido, and mood changes, and are responsible for conducting initial diagnostic investigations and managing associated co-morbidities. GP clinicians initiate the diagnostic process by ordering serum testosterone tests, which should be taken early in the morning when levels are at their peak to account for diurnal variation. If testosterone levels are low, luteinizing hormone (LH)and follicle-stimulating hormone(FSH) tests are essential to distinguish between PH (testicular failure) and SH (hypothalamic or pituitary dysfunction). Additionally measure prostate-specific antigen (PSA) levels before initiating testosterone therapy to rule out underlying prostate pathology and to monitor for any potential side effects, particularly in men over 40. Rising PSA levels during treatment should prompt a urology referral to investigate the risk of prostate cancer. Functional hypogonadism occurs when low testosterone is secondary to chronic illnesses such as obesity, type 2 diabetes, or metabolic syndrome. This is a great opportunity for clinicians to manage co-morbidities through lifestyle interventions and weight management. The use of phosphodiesterase inhibitors such as sildenafil, for erectile dysfunction, are preferred approaches before considering testosterone therapy, given the mixed evidence on its cardiovascular safety in these patients.
Summary Table for Blood Test Frequency and Timing
| Test | When to Conduct | How Often |
| Early Morning Testosterone | Between 7:00 AM and 11:00 AM | At baseline, then repeat within 2–4 weeks if low |
| Repeat Testosterone | After initial low result | Within 2–4 weeks after the first test |
| LH and FSH | After confirming low testosterone | Typically, once, unless further investigation is needed |
| SHBG | When total testosterone is borderline or inconsistent | Once, with periodic repeats if clinically indicated |
Following these testing guidelines ensures accurate diagnosis and helps differentiate between primary and secondary causes of hypogonadism, improving patient outcomes and guiding
When to Refer Patients with Testosterone Deficiency
General practice plays a vital role in managing patients with testosterone deficiency and identifying those who require specialist referral. Key referral pathways include:
Refer to Endocrinology When:
-
- Primary or secondary hypogonadism is confirmed, requiring further investigation or long-term management.
-
- There is unclear aetiology of hypogonadism that requires specialist input.
-
- Patients are unresponsive to lifestyle interventions or testosterone therapy requires ongoing specialist supervision.
Checking PSA Results Before Initiating Testosterone Therapy
PSA (Prostate-Specific Antigen) should be checked before starting or continuing testosterone replacement therapy (TRT). This helps screen for prostate problems, including possible cancer, and provides a baseline for monitoring during treatment. Testosterone can cause the prostate to enlarge and may raise PSA levels slightly. Current evidence does not show that TRT causes prostate cancer, but changes in PSA still need to be taken seriously.
If PSA is abnormal at baseline or rises significantly during treatment, the patient should be referred to a urologist for further assessment to rule out cancer or other prostate conditions, such asbenign prostatic hyperplasia (BPH), prostatitis, orprostate cancer.
PSA Reference Range
A PSA level of <4.0 ng/mL is generally considered normal in men, although age-specific ranges are more accurate.
For men over 60, a PSA of 3.0 ng/mL or higher may warrant further investigation.
Rapidly rising PSA levels, even within the normal range, are also concerning.
When to Refer
PSA >4.0 ng/mL
Age-adjusted PSA thresholds exceeded
Family history of prostate cancer
Abnormal digital rectal examination (DRE) findings
Refer to urology to rule out prostate cancer before starting TRT.
Concerns About Prostate Cancer or Other Prostate-Related Issues
If a patient has prostate symptoms (e.g., difficulty urinating, blood in the urine, or pelvic pain) or a family history of prostate cancer, further investigation is necessary. Testosterone therapy can stimulate prostate tissue, potentially worsening BPH or making latent prostate cancer more detectable.
Key Signs to Watch For:
-
- Urinary symptoms: Frequent urination, nocturia, weak stream, urgency, or incomplete emptying.
-
- Family history of prostate cancer, especially in first-degree relatives.
-
- Previous PSA levels that were high or borderline abnormal.
When to Refer:
-
- Persistent urinary symptoms
-
- Family history of prostate cancer
-
- PSA levels rising rapidly
-
- Abnormal DRE findings
Summary of When to Refer Based on PSA Results
| Scenario | PSA Threshold/Sign | Action |
| Before starting TRT | PSA >4.0 ng/mL or age-adjusted threshold | Refer to urology |
| During TRT | PSA increase >1.0 ng/mL in 12 months | Refer to urology |
| Persistent urinary symptoms | Any concerning urinary symptoms | Refer to urology |
| Family history of prostate cancer | First-degree relative with prostate cancer | Consider referral |
| Abnormal DRE findings | Hard nodule, asymmetry, or irregular surface | Immediate referral |
Management in Functional Hypogonadism:
-
- Treat reversible causes such as obesity, Type 2 diabetes and chronic illness and encourage lifestyle interventions (weight loss, exercise, and stress management) to improve testosterone levels.
-
- Prioritise chronic disease management before considering testosterone replacement therapy.
It’s important to note that over recent years, there has been a surge in testosterone prescriptions for men with sexual dysfunction or perceived age-related decline in testosterone. This trend raises concerns about overdiagnosis and unnecessary treatment. Therefore, a thorough evaluation and confirmation of testosterone deficiency are imperative before initiating therapy.
For men with secondary hypogonadism associated with obesity, chronic illnesses, or metabolic syndrome, lifestyle modifications play a crucial role in improving testosterone levels and overall health. Unlike primary hypogonadism, where the underlying cause is testicular failure and requires testosterone replacement therapy (TRT), secondary hypogonadism can often be improved through targeted lifestyle interventions. These modifications not only improve testosterone levels but also reduce the risk of cardiovascular disease, diabetes, and other chronic conditions.
Practical Recommendations:
-
- Calorie Reduction: Aim for a calorie deficit to achieve sustainable weight loss.
-
- Balanced Diet: Focus on a Mediterranean diet, which is rich in healthy fats, whole grains, fruits, and vegetables. This diet has been associated with better hormone balance and improved cardiovascular health.
-
- Protein Intake: Ensure adequate protein intake to maintain muscle mass during weight loss.
Physical Activity: How often and why is it important to reduce visceral fat
The most effective forms of the most effective forms of exercise to boost testosterone are:
-
- Resistance training (weightlifting)
-
- High-Intensity Interval Training (HIIT)
These workouts are powerful because they build lean muscle and burn visceral fat. Studies consistently show that men who engage in regular resistance and HIIT training experience increases in circulating testosterone and improved metabolic health.
What Is Visceral Fat & Why It Matters
Visceral fat is the fat stored deep inside the abdomen around organs such as the liver, pancreas, and intestines. Unlike fat under the skin, it is metabolically active and behaves like an endocrine organ, releasing hormones and inflammatory chemicals that affect the whole body. Visceral fat (fat stored deep in the abdomen) and testosterone influence each other. As visceral fat increases, it contains more of an enzyme called aromatase, which converts testosterone into oestrogen, leading to lower testosterone levels. This fat also releases inflammatory substances that interfere with the brain–testes signalling pathway responsible for testosterone production, and it is closely linked to insulin resistance, which further reduces the ability of the testes to make testosterone.
Low testosterone then encourages more fat gain, creating a vicious cycle. Reduced testosterone leads to loss of muscle mass, a slower metabolism, increased central fat storage, and lower energy levels, making physical activity less likely. This pattern is often referred to as the hypogonadal–obesity cycle. Clinically, the combination of excess visceral fat and low testosterone is associated with metabolic syndrome, type 2 diabetes, abnormal cholesterol levels, cardiovascular disease, and chronic inflammation. Encouragingly, lifestyle measures such as weight loss, resistance exercise, and improved sleep can reduce visceral fat and help restore healthier testosterone levels, often before medication is required.
The Bottom Line
Lifestyle choices can have a powerful effect on testosterone levels and overall metabolic health. Resistance training helps stimulate natural testosterone production while building muscle, which supports a healthy metabolism. High-intensity interval training (HIIT) is effective at reducing visceral fat and improving insulin sensitivity, both of which help maintain hormonal balance. A Mediterranean-style diet, rich in whole foods, healthy fats, and antioxidants, reduces inflammation and supports hormone function. Getting 7–8 hours of quality sleep is essential because much of the body’s testosterone is produced during deep sleep. Managing stress is also important, as chronically high cortisol (the stress hormone) can suppress testosterone levels. Together, these habits help create an environment where testosterone can be produced and regulated more effectively.
| Intervention | Effect on Testosterone | Practical Recommendation |
| Weight Loss | Increases testosterone levels | Achieve a 5–10% body weight reduction |
| Physical Activity | Boosts testosterone, reduces fat | Resistance training and HIIT exercises |
| Sleep Optimisation | Enhances testosterone production | Ensure 7–9 hours of quality sleep per night |
| Stress Management | Reduces cortisol, improves hormonal balance | Practice mindfulness, yoga, or breathing exercises |
| Smoking and Alcohol Reduction | Reduces oxidative stress and improves testosterone | Quit smoking and limit alcohol intake |
| Managing Comorbidities | Improves overall health and hormone balance | Focus on blood sugar, blood pressure, and cardiovascular health |
Conclusion: Understanding and Managing Testosterone Deficiency
Testosterone deficiency is a complex condition that impacts multiple aspects of physical, psychological, and metabolic health. It can lead to symptoms such as low libido, erectile dysfunction, mood disturbances, fatigue, cognitive decline, and reduced muscle mass. Accurate diagnosis is essential, requiring careful clinical assessment and targeted blood tests, including early morning testosterone levels, repeat measurements, gonadotropin levels, and SHBG to differentiate between primary and secondary hypogonadism.
Management strategies should be tailored to the underlying cause of testosterone deficiency. In cases of primary hypogonadism, testosterone replacement therapy (TRT) can improve mood, cognitive function, bone density, muscle mass, and overall quality of life. However, TRT should only be initiated after ruling out prostate cancer risk through PSA testing and regular monitoring of haematocrit to prevent adverse effects like erythrocytosis. In cases of functional hypogonadism associated with obesity or chronic illness, addressing lifestyle factors such as weight loss, exercise, sleep optimization, and stress management can improve testosterone levels naturally, reducing the need for hormone therapy.
Primary care clinicians play a crucial role in the early identification, diagnosis, and long-term management of testosterone deficiency. They are responsible for conducting diagnostic tests, managing comorbidities, and referring patients to specialists when necessary. Regular monitoring of testosterone levels, PSA, and haematocrit ensures safe and effective treatment, improving both physical and mental health outcomes for patients with hypogonadism. Addressing testosterone deficiency can significantly enhance quality of life, prevent long-term complications, and optimise overall well-being in men and women.